- drsundar@sundarspine.com
- Youtube
For Appointments, Call
+(91) 9080 9680 66
+(91) 9080 9680 66
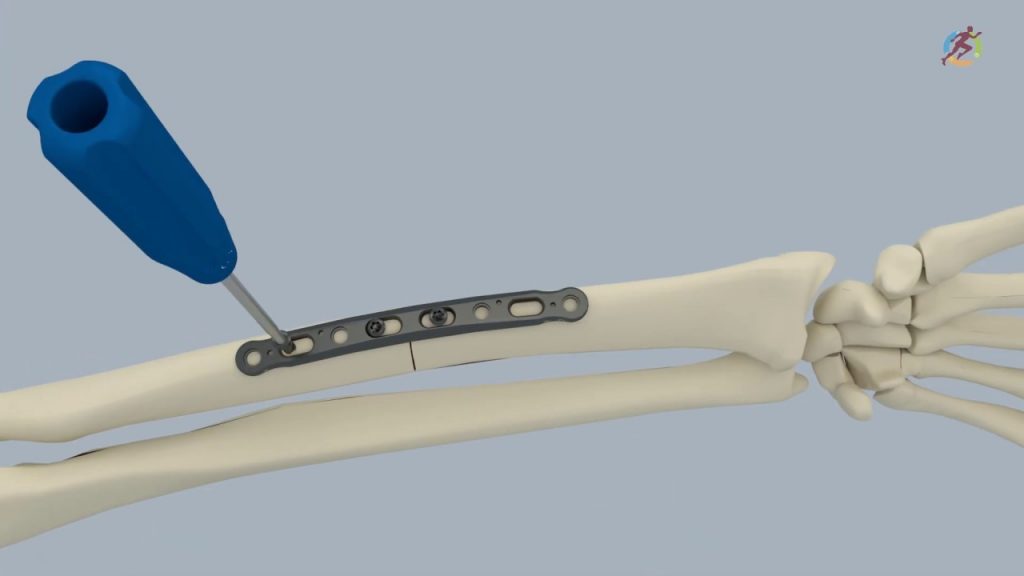
Plate and screw fixation of fracture is one of the most common orthopaedic intervention for fracture management. The procedure involves reducing the displaced fracture fragments and fixing it rigidly by a long linear metal implant (plate) to the bone. Screws are used to facilitate this fixation.
When is this surgery performed?
This is one of the most common and successful orthopaedic surgery, used when:
The surgery is performed by the concept of Open reduction internal fixation (ORIF). The steps involved in any plate fixation are as follows:
Lifting heavy weights is avoided for few days in upperlimb fracture fixation. Weight-bearing is avoided for few days in lower limb fracture fixation.



Intramedullary nailing (IM Nailing) is a technique of fracture fixation commonly used in long bones – thigh bone (femur), Leg bone (tibia) and the arm bone (humerus). This technique has is mainly prefered for weight-bearing bones as they give more stability and support early walking after surgery.
When is this surgery performed?
This technique can be done only in very specific type of fractures:
Advantages of this procedure:
The surgery is performed by the concept of Closed reduction and internal fixation (CRIF). The steps involved in any intramedullary nailing are as follows:


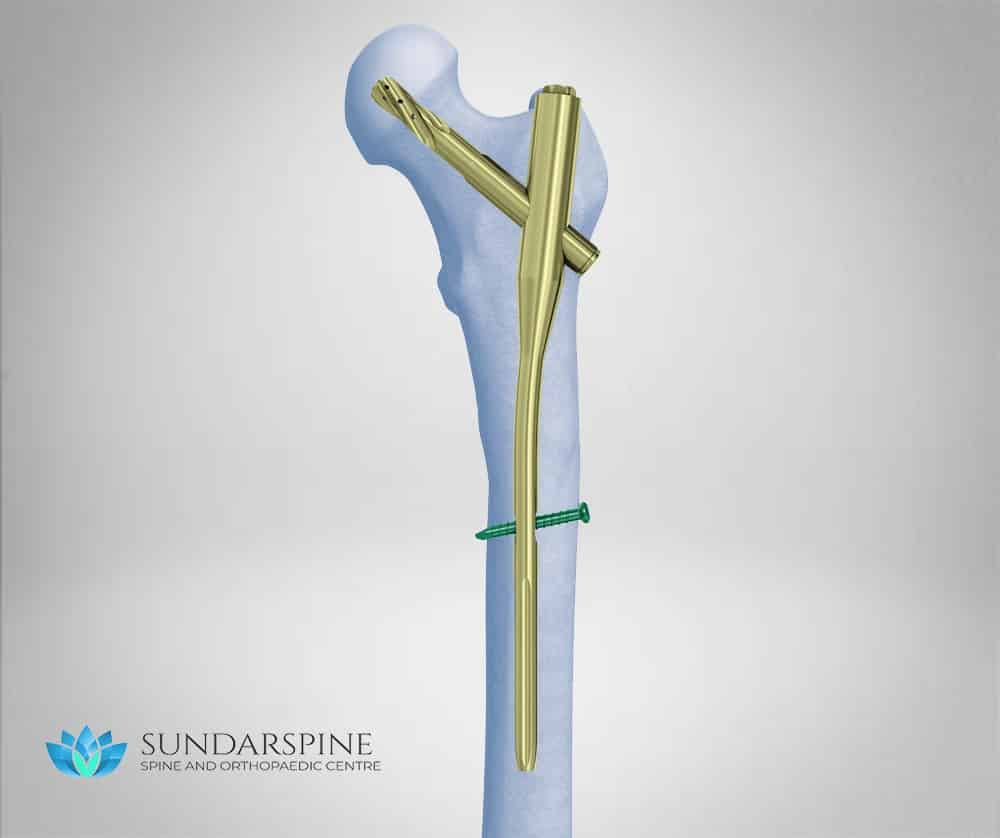
Proximal Femoral nailing is a technique of fracture fixation that is used to treat hip fractures (Proximal femur). Hip fractures are the most common type of fracture especially in the elderly.
When is this surgery performed?
This technique can be done only in very specific type of fractures:
Advantages of this procedure:
The surgery is performed by the concept of Closed reduction and internal fixation (CRIF). The steps involved are as follows:

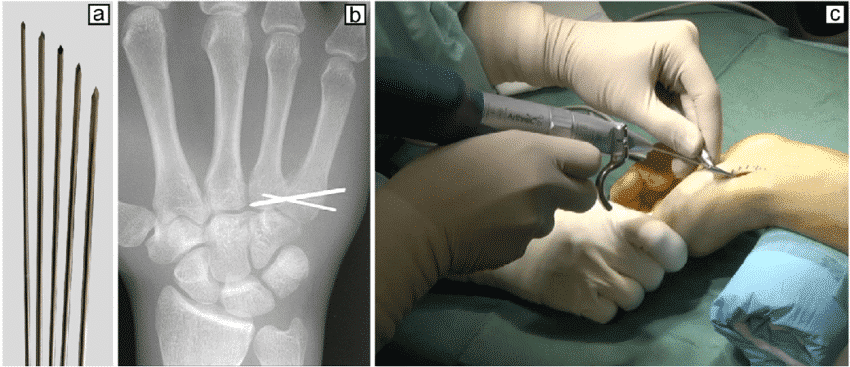
K-wire is a thin metallic pin/wire like structure that is used to fix or stabilize a fracture. They are normally used to fix fractures of the small bones (hands or foot) or larger bones in children. They do not have inherent stability, hence are usually used along with splints or braces till fracture stability.
How the surgery is performed?
The k-wire necessitates removal after 3-6 weeks. The exposed k-wire can be removed in outpatient procedure room whereas the buried k-wire require local/regional anasthesia and hence might be done as an operative room procedure.
Advantages of K-wire:
Holds the fracture fragments in reduced position till the fracture heals. Multiple k-wires increase the stability of the fracture fixation.
Recovery time:
Duration of surgery: 1-2 hours
Walking started: Variable
Hospital stay: 1-2 days
Resume work: After k-wire removal
Brace (Splints): 3-6 weeks
Driving (Car, Bike): After k-wire removal
Strenuous Activity (bending down, lifting weights): Variable


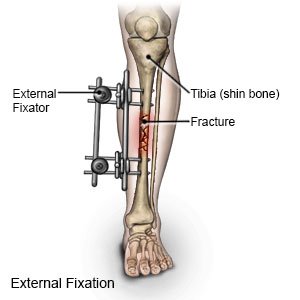
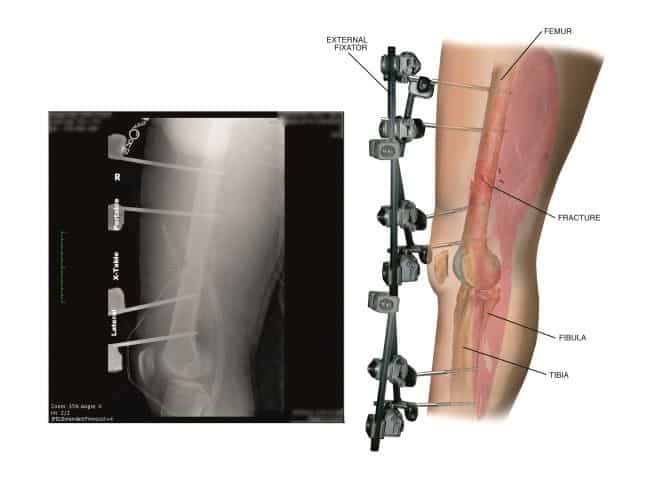
This procedure is usually done in open fracture or in severe multiple injuries to give adequate time for healing before the main final fixation.
When is this Surgery performed?
Advantages of External fixator:
This procedure is usually done as a temporary stabilization till the would and the patient are stable for further procedure. The initial 3 days after a high velocity is a risk period for both the wound (increased swelling, infection) and the patient (risk to life). Hence major procedure such as final fixation are avoided during this period.


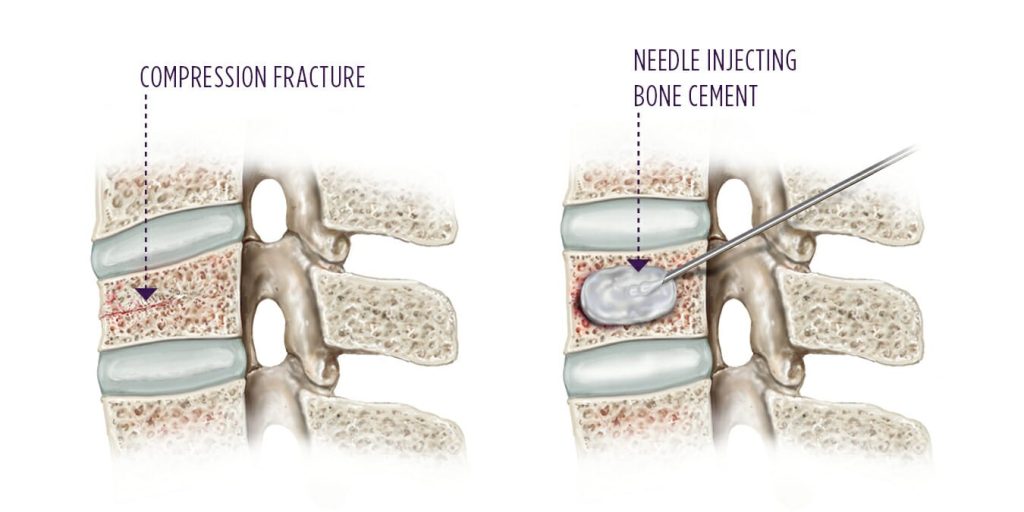
Vertebroplasty is an outpatient procedure for stabilizing compression fractures in the spine. Bone cement is injected into back bones (vertebrae) that have cracked or broken, often because of osteoporosis. The cement hardens, stabilizing the fractures and supporting your spine.
For people with severe, disabling pain caused by a compression fracture, vertebroplasty can relieve pain, increase mobility and reduce the use of pain medication.
When the surgery is performed?
Osteoporotic fracture (more than 60% collapse)
Recovery time:

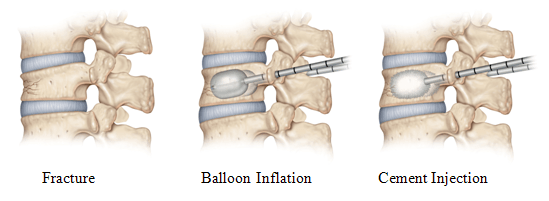
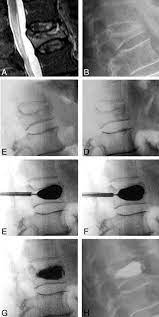
Kyphoplasty is similar to vertebroplasty, but uses special balloons to create spaces within the vertebra that are then filled with bone cement. Kyphoplasty can correct spinal deformity and restore lost height
When the surgery is performed?
Tuberculosis spine, kyphosis deformity, vertebral collapse, tumour spine
Recovery time:
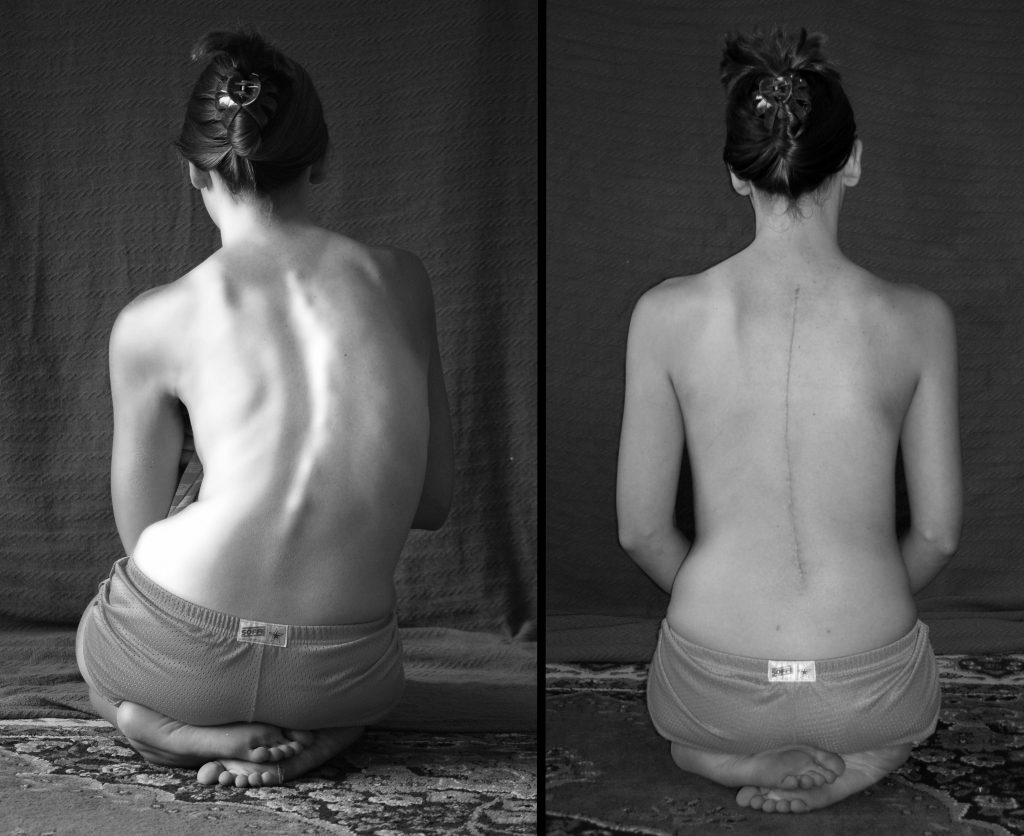
The operation for scoliosis correction is a spinal fusion. The basic idea is to realign and fuse together the curved vertebrae so that they heal into a single, solid bone.
With the tools and technology available today, scoliosis surgeons are able to improve curves significantly.
When the surgery is performed?
The decision to go ahead with scoliosis correction surgery depends on the age of the patient, severity of deformity, secondary cause, curve type and curve progression. However, most scoliosis surgeons agree that children who have very severe curves (45 to 50 degrees and higher) will need surgery to lessen the curve and prevent it from getting worse.
Advantages of Scoliosis Correction:
In severe curves, an anterior surgery might also be necessary and will be performed in the same day or as a 2-stage (alternate day) procedure.
Recovery time:


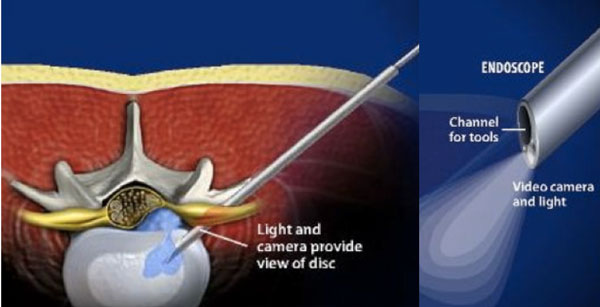
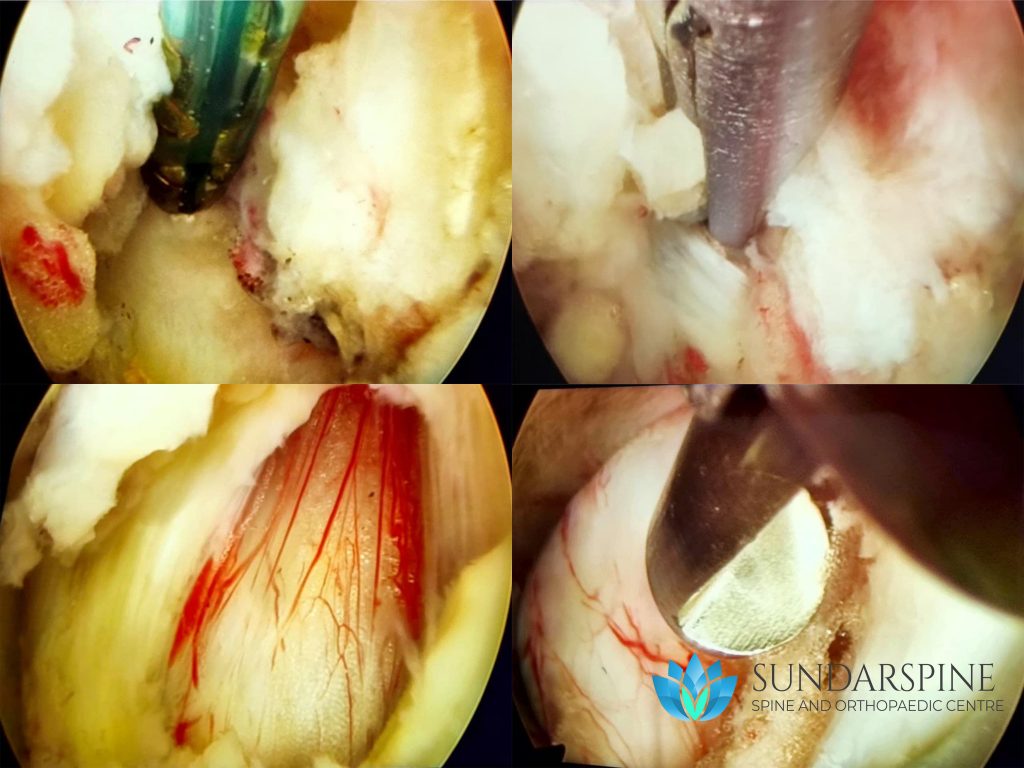
Endoscopic spine surgery is one of the latest advancement in the field of medicine. With the use of a specialized micro-camera and modern crafted instruments, many spine conditions can be treated with a portal (incision) less than 8mm in size.
When the surgery is performed?
Endoscopic spine surgery is mainly performed for Lumbar disc herniation without any significant bone spur or instability.
Advantages of Endoscopic Surgery:
Recovery time: